





COVID-19 in Africa & Yemen: What do seroprevalence surveys tell us?

If you want to contact one of the speakers, you can contact Céline Giustranti + 33 07 87 04 67 89
In December, 2021, confirmed COVID-19 cases from surveillance systems in Africa and Yemen comprised just over 3% of the global burden, despite these countries representing over 18% of the world's population. If correct, this would be an attack rate 6 times lower than the rest of the world (with reported deaths also lower). A lower level of viral circulation might be explained by a younger population or epidemic management practices that allowed for earlier response. But are these hypotheses true, or has the epidemic been underestimated? In 2021, Epicentre conducted seroprevalence and retrospective mortality surveys across different populations (health care workers, refugee camp residents, etc) in Africa and Yemen that provided answers that were quite different from the commonly accepted consensus.
The Art of Choosing the Right Test
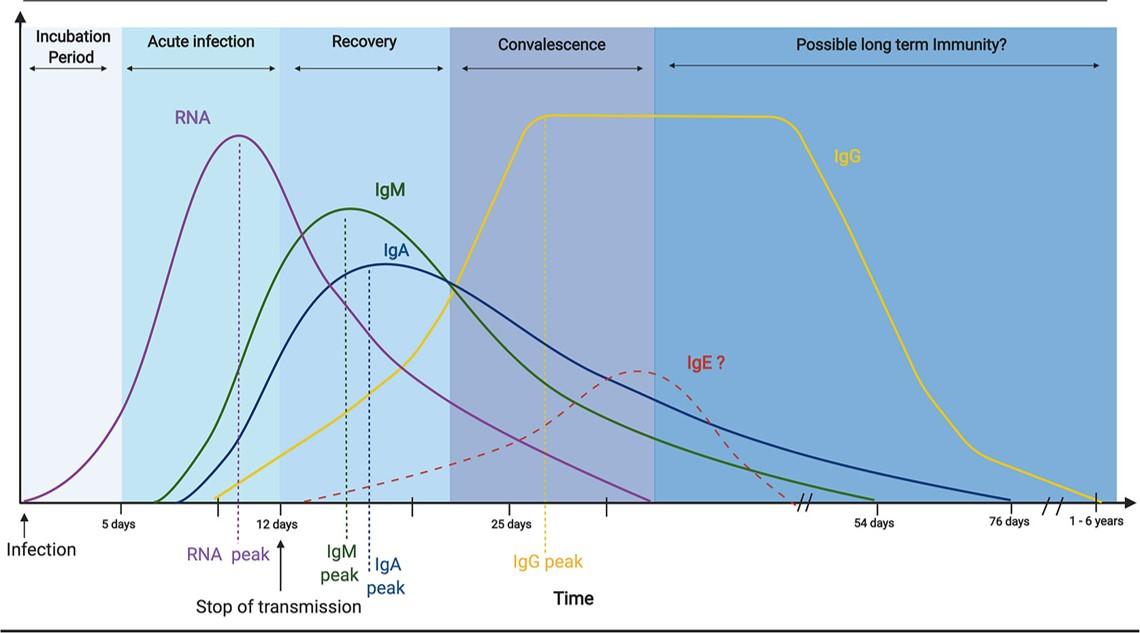
First, a distinction should be made between testing methods. PCR and antigenic tests reveal the presence of virus and make it possible to determine whether a person is infected at the time of the test (whether symptomatic or not). Serological tests look for the presence of an immune response, mainly in the blood, to determine whether a person has been previously infected. Serological tests are based on the detection of immunoglobulin (types M, G, or A – IgM, IgG, IgA) or on a person’s total antibody levels. IgA and IgM are the body’s first line of defense and disappear rapidly. IgG is involved in the body’s memory response and persists for several months. "We mainly looked for IgG in our seroprevalence surveys," says Céline Langendorf, Epicentre's laboratory coordinator. IgGs target different parts of the virus including the spike protein (S), the nucleocapsid (N), or the receptor binding domain (RBD). Some are able to neutralize the virus, or prevent it from penetrating the cell.
In addition to the array of antibodies that can be tested for, there is a wide variety of serological tests available (listed here from the most complex to the simplest: neutralization tests, ELISA or chemiluminescence and fluorescence tests, and rapid immunochromatographic tests or rapid diagnostic tests). These tests vary in ease of use and in sensitivity and specificity.
"Each has advantages and disadvantages that must be taken into account, both when choosing the test that best suits the objectives of the study, and also when interpreting results," cautions Céline Langendorf.
One option is to use very specific methods (to limit the number of false positives), using multiple tests that search for markers of immune response (such as anti-S + anti-N antibodies). "While this highly specific method allows for a minimum seroprevalence estimate, there is a risk of not detecting some true positives and therefore underestimating the impact of an epidemic," notes the biologist. Another option is to choose very sensitive tests, at the risk of overestimating seroprevalence but assuring an accurate description of the population that has been in contact with the virus (even if small), which better assesses the epidemic’s impact.
What is the Epidemic’s Real Magnitude in Africa and Yemen?
Between September 2020 and November 2021, Epicentre conducted seroprevalence surveys in Cameroon, Côte d'Ivoire, DRC, Mali, Sudan, Kenya, Niger and Yemen across multiple target populations. These surveys sought to answer several questions, as Salha Issoufou, Medical and Operations Director of MSF WACa, noted in this webinar’s introduction. Due to a lack of diagnostic testing, fears of a silent epidemic that has nevertheless caused undetected damage remain. The main objectives of the surveys were to assess viral transmission in these populations through seroprevalence testing and to estimate the pandemic’s impact by estimating the excess mortality directly and indirectly related to the virus. For MSF, these seroprevalence surveys should allow operations to make adjustments based on actual risk, to better allocate resources between COVID-19 and high-risk diseases such as malaria or measles, and to identify groups to be targeted in subsequent COVID-19 waves. Because these surveys were conducted in MSF intervention settings and among data-poor populations, they also provide information on the use of rapid diagnostic tests (RDTs), which offer hope for improved diagnosis in hard-to-reach populations.
For health care workers, who are particularly at risk, the presence of past and current infection was investigated by antigenic and serological tests, as well as by identifying COVID-associated symptoms.
- In the Maradi region of Niger, where a survey was conducted from March to April 2021, the estimated seroprevalence was 42% by RDT and 85% by ELISA laboratory testing. Even though this country had reported very few cases of COVID-19.
- In the MSF trauma center in Aden, Yemen where a study was conducted from September 2020 to January 2021, 19% of staff were positive by RDT. Additional subsample screening with an ECLIA laboratory test revealed a much higher seroprevalence of 59%, while RDT seroprevalence had decreased to 8% suggesting a loss of sensitivity over time for RDTs.

For the general population, seroprevalence surveys were nested within retrospective and cross-sectional mortality surveys with cluster sampling. Nearly 15,000 people were tested by RDT. Whenever possible, ELISA/ECLIA tests were also performed. Seroprevalence estimates were:
- 5.8% by RDT in Dagahaley refugee camp in Kenya (between February and March 2021, using a slightly different protocol for security reasons). The number of people infected appears 67 times higher than the number of reported cases. (For more information on the results of the Dagahaley camp, see the publication)
- 34.3% by RDT and 54.6% by ELISA or ECLIA, in Omdurman, Sudan (study conducted from March to April 2021 (for more information: read the preprint)
- 15.7% by RDT and 43.5% by ELISA or ECLIA in Lubumbashi, Democratic Republic of Congo (study conducted April-May 2021),
- 9.6% by RDT in the entire population of Cameroon (study conducted in August 2021), with a high degree of heterogeneity ranging from 4.5% to 17.6% depending on the region,
- The results of studies conducted in two communes of Abidjan in Côte d'Ivoire between July and November 2021 are currently being analyzed.
Notably, findings from a survey conducted by IRD and supported by the African Centers for Disease Control (presented by Antoine Nkuba during the webinar) are consistent with these results, reporting a seroprevalence in Kinshasa (16.6%) higher than the attack rate. This survey was conducted between November 24 and 28, at the beginning of the 2nd wave, using a Luminex technology that allows the detection of antibodies against two antigens (against both the N and S proteins), allowing for estimates of a minimal seroprevalence.
Other notable findings were that seroprevalence increased with age, and that the presence of a COVID positive person in a household was a very important risk factor, with high transmission within households. Across populations, laboratory test results were significantly higher than those obtained with RDTs. However, the risk associated with age, health care work, and household contacts persisted regardless of the type of test used.
“All of the surveys showed infection levels from several dozen to even several hundred times higher than the attack rates of confirmed cases in these countries," says Etienne Gignoux, epidemiologist at Epicentre and coordinator of the surveys. “COVID-positive individuals were also more likely to report having had at least one symptom associated with COVID-19 than COVID-negative people."
In all surveys, an increase in mortality during the pandemic was observed, particularly among people over 50 years old. Although the population involved is younger, COVID-positive individuals report experiencing symptoms. This cluster of indicators suggests a high level of under-detection and under-reporting of cases.
Underestimating the Pandemic and Better Organize Future Response
These surveys found no evidence that the African continent has been spared any greater impact than any other, especially since these surveys were conducted before the waves of delta and Omicron variants. Health care workers and the elderly seem to have been particularly affected.
“The pandemic has had an impact on access to care," says Etienne Gignoux. “The increase in mortality during the pandemic could be the result of a combination of deaths directly and indirectly related to the disease." All surveys noted an increase in death at home. In Dagahaley camp, for example, a reduction of almost a third was seen in consultations and hospital admissions.
Professor Pierre Ongolo-Zongo, Vice-Chair of the National Advisory Group on Immunization in Cameroon, reminds participants that these surveys help to understand the disease in order to organize future response, and that they should guide decisions in terms of vaccine choice. This means that questions surrounding vaccine equality must be asked differently. As Professor Yap Boum, Epicentre's representative for Africa, told Le Monde, "What is the added value of generalized vaccination campaigns (targeting all ages)? We dare to say that some countries may have other public health priorities.” Indeed, the elderly and at-risk population is very small in Africa, which may explain the lower number of reported deaths and questions the relevance of a vaccination campaign that target everyone. General vaccines-for-all-ages campaign strategies could also divert already limited resources in some contexts, whereas targeting at-risk populations (those over-50 and health care workers) in much smaller numbers would be much more efficient. While vaccination of health care workers and the most vulnerable is essential, local and contextualized responses seem necessary for the rest of the population.



