





How can we make epidemiology and medical research more sustainable?

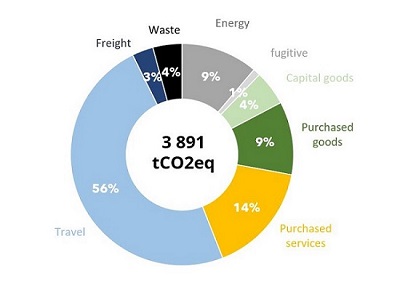 At the end of 2021, Epicentre pledged to reduce its carbon footprint by 50% by 2030, using 2019 as the baseline year. The initial assessment, carried out according to ISO 14064 and GHG Protocol (1) standards, showed that the total carbon footprint in 2019 was 3891 tCO₂e. This footprint came 89% from staff travel (56%), purchasing (23%) and energy consumption (10%). Air travel accounted for a significant share, at 45% of the footprint, and over 11 million kilometers traveled, 80% of which were long-haul.
At the end of 2021, Epicentre pledged to reduce its carbon footprint by 50% by 2030, using 2019 as the baseline year. The initial assessment, carried out according to ISO 14064 and GHG Protocol (1) standards, showed that the total carbon footprint in 2019 was 3891 tCO₂e. This footprint came 89% from staff travel (56%), purchasing (23%) and energy consumption (10%). Air travel accounted for a significant share, at 45% of the footprint, and over 11 million kilometers traveled, 80% of which were long-haul.
First Actions and Roadmap
To achieve its reduction target, Epicentre has drawn up a climate and environment roadmap with the NGO Climate Action Accelerator, comprising 24 concrete measures. These priority actions include reducing the number of kilometers traveled by air, transitioning to renewable energies, implementing stringent environmental purchasing criteria, maximizing the shift from air freight to sea freight to supply its projects, and reducing and recycling waste, particularly single-use plastics.
Focus on Air Travel
Given the importance of air travel in its carbon footprint, Epicentre has focused its efforts on this aspect, in particular by closely monitoring its travel footprint (for the moment excluding training trainee travel, which is included in the 2019 footprint, but for which the organization is not involved). In 2019, these journeys represented 1205 tCO₂ and 7.5 million km travelled. In 2022, these figures fell to 618 tCO₂ and 2.8 million km, and in 2023 to 322 tCO₂ and 1.9 million km. This represents a 75% reduction in kilometers traveled and a 73% reduction in CO₂ emissions, with no reduction in activities.
This spectacular drop can be explained by several factors. Firstly, 2019 was marked by specific events, such as the Ebola epidemic and an Ebola vaccine trial in the DRC, as well as a resurgence of measles in the region, leading to numerous field trips by epidemiologists.
Secondly, situational factor also played a role, such as the restriction on travel to Niger following the coup d'état in the summer of 2023. Finally, structural changes, both individual and collective, have contributed to this decline: strengthening of local skills, limitation of epidemiologist travel linked to changes following the COVID pandemic, reduced physical participation in international conferences, increased use of videoconferencing to maintain interactions, and preferred choice of train for travel within Europe.
Efforts in this direction must continue. For example, a travel policy is currently being finalized, and we're looking into the locations of our training courses. The application developed by Epicentre's Data Science team should help identify the most eco-responsible location depending on where training participants come from, as well as other events.
Optimizing travel and structures
In the Mbarara center in Uganda, a reorganization of recurring trips to the capital and the airport has reduced the number of trips by 30 to 40%. In addition, the purchase of more fuel-efficient city vehicles has helped to limit environmental impact. Analyses are also underway at centers in Niger and Uganda to optimize energy consumption (solar panels, building insulation) and improve waste sorting.
Carbon impact of medical studies
In addition to calculating the footprint by emission source, Epicentre also assessed the carbon impact of two studies:
- a clinical trial on the fractionation of yellow fever vaccine doses (YEFE), which took place over 133 months (including the length of sample storage in Uganda
- a 68-month study (including the length of sample storage) of measles seroprevalence (SeroP) in Niger.
In terms of CO₂e emissions, the YEFE study generated a total of 513 tCO₂e, while the SeroP study produced 43 tCO₂e. In the YEFE study, emissions broke down as follows: 32% attributed to personnel, 15% for laboratory analyses and 24% for travel by personnel (national and international) and participants. Sample storage at -80°C, between freezers and air conditioners, accounts for 10% of the total footprint (or 52 tCO₂e).
For the shorter, less complex SeroP study, 47% (20.6 tCO₂e) of emissions are attributed to long-term storage of biological samples at -80°C, a phenomenon probably accentuated by Niger's heavy reliance on predominantly carbon-based electricity.
Towards sustainable medical research
To limit this carbon footprint, several avenues can be explored:
- Optimizing sample storage:
- Improving building insulation and promoting the use of solar energy
- Reduce storage times and optimize storage sites
- Action on travel:
- At national level: Encourage the use of low-carbon vehicles.
- Internationally: Continue to strengthen local skills and infrastructures to carry out more biological analyses on site, thus reducing international travel.
By approaching our activities through this prism, other solutions should emerge that will complement the 24 listed in the roadmap.
Indeed, the problem needs to be tackled more globally, leading to a rethinking of our practices in terms of epidemiology, medical research and training. This holistic approach, which goes beyond a vision by source of emissions - transport, buildings, waste management - should enable us to find innovative and more sustainable solutions.
(1) protocole international proposant un cadre pour mesurer, comptabiliser et gérer les émissions de gaz à effet de serre
Crédit Photo : Moses Sawasawa

